
( – promoted by Robyn)
 Recently the World Professional Association for Transgender Health released new guidelines for transition related medical care and therapeutic assistance for transgender and gender nonconforming people at a health symposium at Emory University in Atlanta. This is version 7. Version one was written in 1979 by Dr. Harry Benjamin. One of the main changes is its title. Called the Standards Of Care For Gender Identity Disorders in the last version (February, 2001) and all previous versions (1979, 1980, 1981, 1990, and 1998), it is now called the Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People.
Recently the World Professional Association for Transgender Health released new guidelines for transition related medical care and therapeutic assistance for transgender and gender nonconforming people at a health symposium at Emory University in Atlanta. This is version 7. Version one was written in 1979 by Dr. Harry Benjamin. One of the main changes is its title. Called the Standards Of Care For Gender Identity Disorders in the last version (February, 2001) and all previous versions (1979, 1980, 1981, 1990, and 1998), it is now called the Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People.
The sharp-eyed will notice that they dropped the words “Gender Identity Disorder”. I can’t claim to have read every word yet, but I have been informed that the word “disorder” has been expunged. The condition is now referred to as gender dysphoria…which I recall many of us using back in the early 90s (see The Uninvited Dilemma: a question of gender by Kim Elizabeth Stuart.
My own feelings are not out of line with those of Sebastian and Annika at Autostraddle.
The SOC is a very important document for transpeople and their healthcare providers, consisting of the non-mandated (but generally closely followed) standards of treatment for transpeople by those who provide us services. Too often they have been thought to be carved in stone by some of our providers.
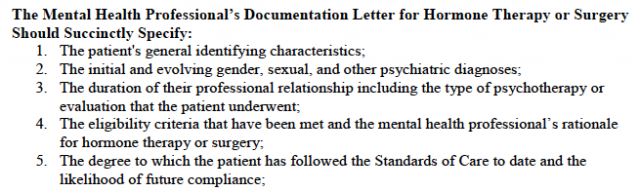
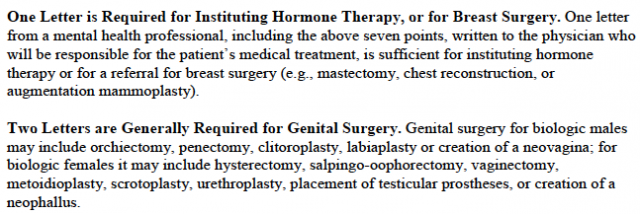
Among other items, the previous SOC specified what was necessary for a patient to receive hormone treatment and/or surgery. A letter was required from a mental health therapist to a physician before hormone treatment could be commenced.
 |
 |
There were also timetables for when such letters could be written.
The requirement for the letters and the timetable are both gone. Someone has apparently realized that many of us are adults and should be able to make these decisions based on informed consent.
That’s how my therapist and my first doctor did it. In fact, I understand that they discussed me at a party both had attended. I had hormones within 40 days of my first meeting with my therapist. I’ve always felt a little guilty about that. I also felt guilty about the fact that I wrote one of my surgery letters and gave it to my second therapist to sign.
Why did we put up with the old SOC? We had to do so in order to get treatment…because the providers mostly acted like gatekeepers.
The requirement for living at least three months in “real life test” (i.e. living openly as the target gender) without hormonal intervention was not only cruel and unusual punishment, it put us in severe danger from the surrounding public.
My discomfort with my own body was increasing by the day. I wanted to cry every time that a stranger addressed me as “sir.” The prospect of having to wait several months before alleviating this pain was really distressing. To be honest, I don’t think that I could have done it.
–Annika
But she did…after first finding a clinic that operated under informed consent. Too often we see people self-medicating with hormones purchased online or going to pumpers, who will shoot us up with just about anything for a buck (ok…many bucks).
For some reason, I thought they were here to stay for a while. Perhaps I had internalized some of the pathologization and saw WPATH as my governing body, as an institution that had the right to govern my body and others. I am currently in the process of applying to Counseling Psychology PhD programs and my big push in my personal statement and desired research directions is that we have no research on effective counseling and psychological “treatment” of people suffering from gender dysphoria, no accepted standards of therapy, and very little professional training in the area, yet we mandate that therapy be a process before these people can transition!
–Sebastian
Therapy is no longer a requirement in the new version, though possibly a good idea, given the maltreatment most of us experience by the society in which we live…especially during transition. There is also no longer a set period of time living in the target gender.
Wouldn’t it be great if we could get some folks to read and understand the following?
A disorder is a description of something with which a person might struggle, not a description of the person or the person’s identity. Thus, transsexual, transgender, and gender nonconforming individuals are not inherently disordered. Rather, the distress of gender dysphoria, when present, is the concern that might be diagnosable and for which various treatment options are available. The existence of a diagnosis for such dysphoria often facilitates access to health care and can guide further research into effective treatments.
Especially it would be nice if it would be read and accepted by the people who edit the DSM (Diagnostic and Statistical Manual of Mental Disorders). I’m not going to hold my breath given the current make-up of that committee.
The DSM-V is on track to be remembered for how the responsible parties reinforced and even expanded the pathologization of sex and gender minorities, rather than taking the courageous and historically inevitable step of depathologization.
—Andrea James, Transsexual Road Map
It’s awful for adults. It’s worse for children, where the point of therapeutic intervention is akin to reparative therapy. The hope for the intervention is to reduce the chance of transsexualism as an adult.
Let the children grow up to be themselves.
The diagnosis of GID in children, as supported by Zucker and Bradley, is simply child abuse.
–Phyllis Burke, author
Worse, “disorders of sex development” are likely to find their way into into the DSM, which would label intersex people as having a mental disorder.
was inevitable that DSD would make its way into these revisions, since the term is such a huge step backwards for sex minorities. That this disorder is intermingled with gender minorities in these proposed revisions was also inevitable. From the moment I heard the term “disorders of sex development” being bandied about by self-styled ethicists, I know this is where we would end up. Their short-sighted advocacy will now result in a generation of people with natural human variations in sex anatomy to be de facto mentally disordered as well as physically disordered. This term implies that these people have a form of retardation (developmental disorder), and we will see an uptick in “cures” for both fetuses and neonates thanks to the term DSD.
–Andrea James
Because of the immenent revision of the DSM, WPATH included intersex in SOC VII. This has not gone down well with interest folks.
WPATH would not formulate a Standards of Care for trans people without considerable trans inclusion and widespread trans consultation.
That WPATH is prepared to do what they have done to intersex people shows the complete misunderstanding that trans professionals have in respect of intersex and their disregard for both our rights and for our wellbeing.
—Gina Wilson, Organization Intersex International Australia (OII)
1. Most of the versions of the SOC had no input from transpeople.
2. I don’t disagree.
One place where we can see the changes possibly helping is with incarcerated transpeople. Although an inmate in California recently had her request for surgery denied, that decision is apparently not the last word.
The US Bureau of Prisons, as part of a court settlement, is adopting new rules. The BOP’s “freeze frame” policy is no more. That policy allowed transgender inmates to only receive such medical care as they had received prior to incarceration.
Vanessa Adams, originally detained in Florida but since moved to North Carolina, sued the BOP in 2009 after being denied hormone replacement surgery…since she had not been on HRT before her conviction. Prison medical staff diagnosed her with Gender Identity Disorder, but did not treat it. Adams became depressed…to the point of first attempting to perform self-castration with a razor…and ultimately succeeding in amputating her penis.
In June a federal judge ruled in favor of Adams. The two sides were sent to mediation. The new policy is the result of that mediation.
The [new] treatment plan may include elements or services that were, or were not, provided prior to incarceration, including, but not limited to: those elements of real life experience consistent with the prison environment, hormone therapy and counseling.
–Newton Kendig, BOP medical director
The memo from Kendig also states that widely accepted practices for treating transgender patients should be used by prison medical and mental health staff.
That could be read to include the possibility of gender confirmation surgery provided prison doctors agree it was necessary for an inmate.
The memo is dated May 31 and was sent to all 116 federal prisons. The public announcement was just this past Friday.
Personal advice? I don’t believe any transperson should commit a federal crime just to see if they can get surgery.
One other recent story
A day after an advisory panel studying Medicaid in New York floated the idea of having transgender surgery covered, Governor Cuomo’s health department decided that wouldn’t be politically prudent.
No consideration is being given to any change in current state policy and any proposal to have gender reassignment surgery funded by Medicaid would be rejected.
California and Minnesota do use Medicaid funds for GRS.
Many people…maybe even a majority around these parts…would be opposed to funding GRS with Medicaid money. The claim is usually that it is just elective, cosmetic surgery.
And it would be only cosmetic surgery…for someone who wasn’t transsexual.
3 comments
Author
…the High Court of Australia has ruled that two transmen can be legally recognized as men even though they still have some female parts.
Hear that everyone? You cannot see our chromosomes and we really don’t hope you see our genitals when we are in public (that would be the people wearing their pants down below their butts), so you go by what you see.
The Gender Reassignment Board of western Australia had said they externally look like men and they say they are men, but would not certify that they were men because they still had some female reproductive systems.
The High Court unanimously reversed that decision.
So if you are talking to someone’s breasts, that person is a woman regardless of what is in her pants.
I book marked them for thorough reading tomorrow while I’m in the ER and can do a little in house teaching. It will certainly be an education for the residents in the little ER where I work, even a fews of the attendings. I love teaching moments. 🙂