
(2 pm. – promoted by ek hornbeck)
While the silence from most of US mainstream media remains deafening, the print and online news publication for physicians published by the American Medical Association – American Medical News – reported yesterday May 16 that Vermont Governor Peter Shumlin has scheduled a bill-signing ceremony for May 26 during which he will sign a bill approved by the Vermont Democratic-controlled legislature, with the state Senate voting 21-9 to pass it on May 3, and the House adopting it on May 5 with a 94-49 vote “that paves the way for the state to launch a health system approaching a single-payer model later in the decade and to create a state health insurance exchange”.
The measure creates a powerful five-member Green Mountain Care Board, members of which will determine the benefits and craft a funding plan for Green Mountain Care, a state universal health plan. The board would have wide authority over state health spending and health system reform. The bill requires the governor to nominate Green Mountain board members by Oct. 1 and the Vermont Senate to confirm them.
All Vermonters would be eligible for the plan, which would cover hospital services and prescription drugs.
Shumlin had pledged to enact a single-payer health system during his January 6 inaugural address, saying “Let Vermont be the first state in the nation to treat health care as a right and not a privilege.“
The rising cost of healthcare for Vermont’s middle class and small businesses provides an equally daunting threat to economic prosperity. Just ten years ago our little state was spending $2.5 billion a year to stay healthy. Today we spend over $5 billion. That increase represents an enormous hidden tax on families and small businesses across our state. If left untethered, the rising cost of health insurance will cripple us.
That’s why we must create a single-payer healthcare system that provides universal, affordable health insurance for all Vermonters that brings these skyrocketing costs under control. Let Vermont be the first state in the nation to treat healthcare as a right and not a privilege; removing the burden of coverage from our business community and using technology and outcomes-based medicine to contain costs. By doing so, we will save money and improve the quality of our care.
Some will say it can’t be done. The special interests; insurance companies, pharmaceutical industry, medical equipment makers; the same lobbyists that spent hundreds of millions of dollars to make sure that real reform withered in Washington can be expected to exercise their will to protect their enormous profits.
Shumlin went on in his inaugural address to make clear that the current systems of private health insurance is a job killer:
Others will say reform will destroy our existing healthcare system. But logic suggests – and our experience shows – that our current system is unsustainable; that underfunded reimbursements starve our doctors and hospitals; that duplication, waste, inefficiencies and rising costs will drive more rural providers into bankruptcy and destroy our quality of care, which is the very best in the land. I ask the defenders of the current system to explain how small businesses, municipalities and taxpayers can sustain double digit premium increases year after year.
The AMN article notes that:
The measure approved by the Legislature has three major parts:
- The Green Mountain Care Board, a five-member panel appointed by the governor with Senate confirmation. The board would design the state’s universal coverage plan, develop state health care budgets, and carry out health cost containment and payment reform.
- The Vermont Health Benefit Exchange, a state marketplace for health insurance as called for under the national health system reform law. The exchange would start operating by 2014 and could become the main source of health coverage in Vermont by 2017.
- Green Mountain Care, the state’s universal coverage plan, which could launch by 2017. The state would need federal approval to use federal health funds to help finance the plan. The state is expected to adopt payroll or income taxes to help pay for the plan.
…and goes on to note that:
the bill does not meet the strict definition of a single-payer plan, in which the government is the sole third-party payer for health care. “But it is as close as we can get at the state level,” said bill sponsor [Vermont Rep. Mark] Larson.
The measure would allow private health plans to continue in the state indefinitely. “You give up a significant part of the administrative savings by doing that,” said David Himmelstein, MD, founder of Physicians for a National Health Program. The organization, based in Chicago, advocates for a single-payer health system.
A true single-payer plan should have separate operating and capital budgets, Dr. Himmelstein said. It should require a single insurance fund to pay all claims, he said.
Green Mountain Care – greenmountaincare.org – is the official State of Vermont website for health insurance. It includes plans such as Catamount Health, Vermont Health Access Plan (VHAP), Dr. Dynasaur, Medicaid, and a number of pharmacy assistance and premium assistance programs.
Plan eligibility and cost is based on household size and income. There may be a program for you, no matter how much you earn. Call 1-800-250-8427 or complete the Green Mountain Care Screening Tool to find out which plan is right for you!
Each program has different eligibility requirements. Eligibility for these programs is based on your application. You do not need to apply for a specific program. We will screen you for the health care program for which you are eligible.
Click here to learn more about eligibility, covered services, and the cost of each Green Mountain Care plan.
Vermonters who need long-term care services may qualify for financial assistance through Choices for Care – Vermont’s Long-Term Care Medicaid Program. Click here to go to the Department for Children and Families’ website for details about the program and how to apply.
Hopefully the new Vermont plan will begin the same kind of momentum for the U.S. that led to the development of true national single payer health care in Canada, and go a long way towards redressing the inequities Holly Dressel illuminated forcefully in a 2006 Yes Magazine article…
Publicly funded health care has its problems, as any Canadian or Briton knows. But like democracy, it’s the best answer we’ve come up with so far.
Should the United States implement a more inclusive, publicly funded health care system? That’s a big debate throughout the country. But even as it rages, most Americans are unaware that the United States is the only country in the developed world that doesn’t already have a fundamentally public–that is, tax-supported–health care system.
That means that the United States has been the unwitting control subject in a 30-year, worldwide experiment comparing the merits of private versus public health care funding. For the people living in the United States, the results of this experiment with privately funded health care have been grim. The United States now has the most expensive health care system on earth and, despite remarkable technology, the general health of the U.S. population is lower than in most industrialized countries. Worse, Americans’ mortality rates–both general and infant–are shockingly high.
…
The United States spends far more per capita on health care than any comparable country. In fact, the gap is so enormous that a recent University of California, San Francisco, study estimates that the United States would save over $161 billion every year in paperwork alone if it switched to a singlepayer system like Canada’s. These billions of dollars are not abstract amounts deducted from government budgets; they come directly out of the pockets of people who are sick.
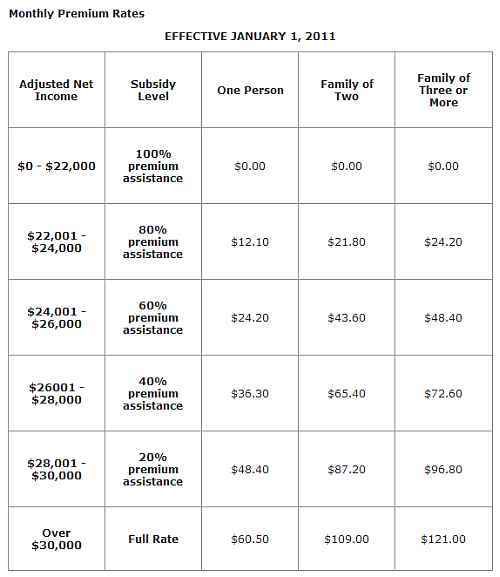
British Columbia is one of three of the ten Canadian Provinces that charges a monthly premium for health insurance. In the other 7 provinces there is no monthly premium – the entire program is covered from general tax revenues.
Also, in British Columbia,
there are two premium assistance programs that offer subsidies to those in financial need: regular premium assistance and temporary premium assistance.
Regular Premium Assistance
Effective January 1, 2010, the regular premium assistance program was enhanced to allow more British Columbians to qualify and to allow persons already receiving a partial subsidy to qualify for a higher level of assistance.
Regular premium assistance offers subsidies ranging from 20 to 100 per cent, based on an individual’s net income (or a couple’s combined net income) for the preceding tax year, less deductions for age, family size and disability. The resulting amount is referred to as “adjusted net income”. See the Monthly Premium Rates chart below for details of premium assistance rates.
In 2004 Morton Mintz writing for The Nation put together a very long and exhaustive analysis of the economic impacts of single payer health care, stating among other things that:
Publicly financed but privately run healthcare for all–including free choice of physicians–would cost employers far less in taxes than their costs for insurance. Universal coverage could also work magic in less obvious ways. For example, employers would no longer have to pay for medical care under workers’ compensation, which in 2002 cost them more than $38 billion. Auto-insurance rates would fall for them–and everyone–if the carriers were no longer liable for medical and hospital bills. You’d think that in its own selfish interest, Corporate America would be fighting to replace the existing system with universal health coverage. Yet it doesn’t lift a finger.
[snip]
“Double-digit increases in healthcare costs are a drag on economic growth,” says Henry Simmons, president of the National Coalition on Health Care, an alliance of groups working for healthcare reform. They “slow the rate of job growth,” “suppress wage increases for current workers,” “undercut the viability of pension funds,” “put American firms at a steep disadvantage in world markets” and produce “severe long-term budgetary problems” for the federal and state governments.
Two unrelated but mutually reinforcing reports coming out on a single day, August 19, validate the economic-drag theory. First was a study that found a “relationship between job growth and health-care costs” in eighteen industries between 2000 and 2003. It was done for the Kerry campaign by Sarah Reber, assistant professor of policy studies at the University of California, Los Angeles, and Laura Tyson, dean of the London Business School and former head of President Clinton’s Council of Economic Advisers and National Economic Council. The evidence, the authors write, “suggests that employers have reduced hiring in response to rising health insurance premiums,” and that rising premiums have led to a deterioration in the quality of jobs. In industries where health-insurance benefits accounted for a comparatively large share of total employee compensation, job growth was slower than in industries where they accounted for a smaller one. Thus, in the accommodation and food services industry, “benefits constituted about 12 percent of total compensation for workers…and jobs grew…by about 2.5 percent. In manufacturing…the benefits share was 18.5 percent and job losses topped 18 percent.” [Emphasis in original.]
This picture was reinforced by a New York Times article based on “government data, industry surveys and interviews with employers big and small.” It said:
employers big and small…remain reluctant to hire full-time employees because health insurance, which now costs the nation’s employers an average of about $3,000 a year for each worker, has become one of the fastest-growing costs…. Health premiums are sapping corporate balance sheets even more than the rising cost of energy.
[snip]
Canada has had a single-payer system for more than thirty years. (Australia, Denmark, Finland, Iceland, Sweden and Taiwan also have one.) American executives who have run Canadian subsidiaries see it as a business boon. Take General Motors. In 2003 its costs of building a midsize car in Canada were $1,400 less than building the identical car in the United States (the comparable figures for DaimlerChrysler and Ford were $1,300 and $1,200). Such savings are no mystery. Canadian companies pay far less in taxes for health coverage for everyone than the premiums they would pay under the US system to provide their employees with comparable benefits.
Highly placed Canadian business executives affirm that single-payer nurtures free enterprise. A. Charles Baillie, while chairman and CEO of Toronto Dominion Bank, one of Canada’s six largest, hailed it in 1999 as “an economic asset, not a burden.” He told the Vancouver Board of Trade, “In an era of globalization, we need every competitive and comparative advantage we have. And the fundamentals of our health care system are one of those advantages.” He added: “The fact is, the free market…cannot work in the context of universal health care. While health care could be purchased like any other form of insurance…the risk and resource equation will always be such that, in some cases, demand will not be matched by supply. In other words, some people will always be left out.” (A recent report by the World Bank ranked welfare states like Denmark, Finland and Sweden high in international competitiveness. An author of the study said, “Social protection is good for business, it takes the burden off of businesses for health care costs.”)
In 2002, top executives of the Big Three automakers’ Canadian units joined Basil (Buzz) Hargrove, president of the Canadian Auto Workers (CAW) union, in signing a “Joint Letter on Publicly Funded Health Care.” At a press conference with Hargrove, Michael Grimaldi, president and general manager of GM Canada and a GM vice president, called single-payer “a strategic advantage for Canada.” The joint letter, also signed by Ford’s and DaimlerChrysler’s presidents and CEOs, Alain Batty and Ed Brust, said that while providing “essential and affordable healthcare services for all,” single-payer “significantly reduces total labour costs… compared to the cost of equivalent private insurance services purchased by US-based automakers” and “has been an important ingredient” in the success of Canada’s “most important export industry.”
[snip]
Corporate America is blowing a supreme opportunity to do well by doing good. Enlightened self-interest this is not.
……….
Read it all here…
Single-Payer: Good for Business
Morton Mintz, The Nation, October 28, 2004
2 comments
Author
the only Republican to vote for the bill…
Or as some call it – RomneyCare. Which happens to be almost the same as ObamaCare.
MassHealth was a bit difficult to get started but it works excellently when you are in. Like any major insurance plan there are variations on doctors and prescription drugs.
The huge difference is when you have to get on the phone to someone in the MassHealth bureaucracy, they are friendly and do anything they can to help you. I’ve found private insurance does anything they can to block you.
My advice – take single payer any day. The hassle level is lower than private insurance.