
(noon – promoted by Nightprowlkitty)
The psychedelic amphetamines (and I include mescaline here, although it is a methyl group away from being a true amphetamine) are many and widely encountered in what are almost always now illicit settings. They (except for mescaline) are synthetic drugs, not found in nature and can be decided with a 5 panel drug test.
These drugs are “true” psychedelics as opposed to the oddballs described here last week. Many of the oddballs are dissociatives, and the true psychedelics work by a completely different mechanism.
Before we get started, a bit of housekeeping. I STILL have not bought cigarettes since March. I noticed at my old brand, Camel nonfilters, are now $6.28 a pack, or around $60 a carton. I am still smoking, but the Prince Albert and Top leaves cost about $0.40 per pack. Now that I am used to them, I do not think that I am in danger of relapsing to Camels. The next step is to begin rationing, and I think that I will count out a given number of cigarette leaves and not rolling another cigarette after my allotment is exhausted for the day, then to reduce my allotment once a week. I shall keep you posted.
On a second note, many of you know that I collect coins. Yesterday I found a 1964 Philadelphia cent, double die reverse, FS-01-1964-002, CONECA 58-R-II. In AU-50 to MS-60, it is probably worth $30, give of take.
Now, to the subject at hand. There is an extremely important neurotransmitter in the body called 5-hydroxytryptamine ( 5-HT), also known as serotonin, that controls a number of functions. Here is a picture of 5-HT (this will become even more interesting next time):
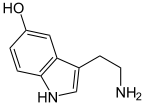
Serotonin (5-HT)
There are at least seven families and many subtypes of 5-HT receptors, but the specific one that seems to have to do with psychedelic effects is the 5-HT2A one. (By the way, I can not get the HTML for subscripts to work. The superscript one is fine, but the subscript just displays as the HTML code. Anyone able to help?) 5-HT itself is an agonist for all families of receptors, whilst the psychedelics are specific, more or less, for the 2A one. The 5-HT system in turn affect the functions of many, many other neurotransmitters (and other materials) in the body. Functions as diverse as nausea to sleep to mood to bowel function are regulated by the various 5-HT receptors. If fact, the reason that narcotics (my previous post on them is here) work by being antagonists to the 2B and 2C subtypes and the 3 and 4 families.
In any event, all “true” psychedelics bind to and strongly activate (that is are at least partial agonists) of the 5-HT2A receptor. This has been shown by classical methods such as radioactive labeling, and by more modern methods, so it is pretty well established. Now, 5-HT is also deeply involved with mood, and the newer antidepressants work by preventing the reuptake of serotonin by presynaptic neurons in cases of depression. More serotonin, better mood. It might be informative to review the introduction to this series here if you are not hip to neurobiology. (In the last installment of this series, I shall a complete list of links to previous ones).
Some psychedelics bind to other receptors as well, and also have stronger or weaker binding to the 5-HT2A one, accounting for different subjective effects for different drugs. Not all of these interactions are well known, but a few are and I shall point them out as we discuss particular drugs if that information is known. Another observation that I would make is that, although a great deal of study has been done on many of these drugs, not everything hypothesized is yet proven.
The prototypical drug of this class is, as I said, not an amphetamine at all. It is mescaline, used for centuries in Native American rituals. It occurs in several members of the cactus family, Cactaceae. In North America it is found in the peyote cactus, Lophophora williamsii, and in South America in the Peruvian Torch (Echinopsis peruviana) and the San Pedro (Echinopsis pachanoi) cacti. Traditional use of the drug is as an entheogen, an agent to make one feel or relate to god within the person. Used in these settings, there seems to be some benefit in a spiritual way (for instance, in treating alcohol overuse).
Here is a structural formula for mescaline. It is not an amphetamine because it lacks a methyl group on the carbon connected to the nitrogen, but it pretty darned close:
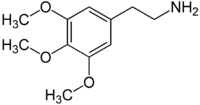
Mescaline
As a drug of abuse, mescaline seems to be fairly harmless insofar as physical effects go. Since it often causes nausea, especially in higher doses, it is fairly difficult to overdose on it. It is not a particularly potent drug, as psychedelics go, requiring half a gram of pure drug for hallucinatory experiences to occur. It lasts for about 10 to 12 hours, give or take, depending on the dose and the individual. Since it is structurally similar to the amphetamines, stimulation of nervous system is also observed due to its mimicking of norepenepherine. The installment on amphetamines goes into detail about the mechanism for that.
Mescaline is notable for its vivid visual distortions, particularly the geometric shapes imagined. Southwestern Native American art is thought to be strongly influenced by these visions. Here are a couple of examples:




Mescaline is a Schedule I drug in the United States, meaning that it can not be possessed or manufactured for any reason unless one has a DEA license permitting it. This effectively shuts off medical research except for a very few institutions without a DEA license.
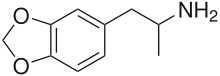
The psychedelic that is probably most popular at present is MDMA (methylenedioxymethamphetamine), or Ecstasy. This could almost have been in last week’s oddballs section, but it is more like classic psychedelics than it is the oddballs. Here is a structural diagram:
MDMA
Note that it has some carbon-oxygen chicken fat (a highly technical term that we organic chemists use to describe groups that are not part of the central skeleton of a molecule) attached to the ring like mescaline, and unlike mescaline has a methyl group on the carbon in the chain next to the nitrogen, making it a true amphetamine.
MDMA only weakly agonizes the 5-HT2A receptor, so the hallucinogenic potential is less than for other psychedelics, but some disturbances still exist. The most notable feature of this drug is the heightening of mood and feelings of warm feelings towards others. It also has many of the effects of the amphetamines (link above).
It is suggested that the production of warm feelings (drugs that do that are called emphathogens, also called entactogens) has to do with the fact that MDMA causes a release of the hormone oxytocin due to agonism of the 5-HT1A receptors. It is known that oxytocin, in addition to its physical actions, has powerful effects on bonding, generosity, and trust. This goes a long way to explain this effect.
The mood elevation is explained by the rather unique ability of MDMA to release large amounts of 5-HT itself. This floods the synaptic junction with H-HT, strongly elevating mood and giving feelings of well-being in addition the the oxytocin ones. But there is a cost, as I will develop in the next few paragraphs.
There are a number of health hazards associated with MDMA, some acute and some chronic. The acute ones seem to have to do with the amphetamine part of the molecule. It is a stimulant, and speeds up the metabolism. It is also an appetite suppressant, reducing the desire for food. Most of the acute effects of this drug have to do with this and in the way that it is used.
Early in the 1960’s the concept of set and setting was developed for the responsible use of psychedelic drugs. Set refers to the mental readiness to undergo the psychedelic experience, such as anger and other negative emotions (that need to be minimized to reduce the probability of a bad trip) along with other emotional issues. Everyone has a different set, and it changes depending on long term and recent experiences. Setting refers to the actual physical place that the drugs are used, such as a familiar room with comfortable furniture and trusted people, a peaceful park or woodland, or, on the other extreme, an environment that itself causes anxiety, such as a loud crowd.
The popular use of MDMA optimizes neither set nor setting, and, fortunately it is just a weak 5-HT2A agonist, or the rave scene would be even worse than it is for users. When used by responsible mental health professionals, subjects were (since it is Schedule I now, very rarely are) counseled about the goals of the therapy, the effects of the drug, and what was to be expected, both immediately and long term. Thus, a positive set was established. The drug was administered in a quiet, peaceful, and supportive place that was designed not to cause undue anxiety, establishing a positive setting. Under those conditions, this drug shows many promising possibilities for mental health therapy. For example, it seems to be quite good at helping couples who have issues and have grown apart to reconnect, probably from the oxytocin release since, as I indicated above, has to do with bonding. This seems to work only if both individuals want to reconnect. It has shown some advantage in the treatment of alcohol abuse and other conditions for reasons not completely understood.
Additionally, under such controlled conditions any medical difficulties can be dealt with right away, and the dosage is carefully controlled. MDMA, like mescaline, is relatively nonpotent, so a large dose (150 to 300 milligrams) has to be taken. This means that the amphetamine part of the molecule is pretty much the culprit in overdose. MDMA tends to raise core body temperature from its amphetamine aspect. It also stimulates antidiuretic hormone, which tends to reduce urine output, but still pulls sodium out of the body, just in a smaller than normal volume of urine. Since the bladder tells one that it is ready to be emptied by the pressure within it, this can lead to sodium depletion because of small volume of very sodium enriched urine. Sweating, another sodium loss mechanism, is increased under the influence of this drug.
Now let us look at the rave situation. The set is one of the expectation to “get off”, and little more unless I am very much mistaken. Anyone who has a friend that believes otherwise is welcome to post a comment that I will consider. The setting could not be worse. Loud music, lots of movement, and lots of people do not contribute to an introspective experience, essential to the therapeutic use of the material. At the rave, music is loud, people are plentiful, and movement is extreme. This causes several problems at once.
The loud music and motion exacerbates the 5-HT2A part of the experience, causing some hallucinations, but not as marked as those of “stronger” psychedelics. More importantly, the dancing and close quarters raise core body temperature, making a hyperthermic crisis (heatstroke) more likely, especially because of the amphetamine moiety causing hyperthermia anyway. Add to that the pressor effects (blood pressure and heart rate increase), and the sweating out of sodium, and the concentration of sodium in the urine, and there is a disaster in the making. Many MDMA ravers get thirsty, but do not want food. So they drink plain water, and the sodium elimination is accelerated. This does not happen very often, fortunately, but it does happen. Almost all of the fatalities involving MDMA have occurred at raves, or shortly after the subject leaving one, and involved either hyperthermia, hyponatrimia (low sodium), or both.
There are a couple of other problems associated with the rave scene. One is that it can not be possible to know the dosage, let alone the identity of the drug purchased. It might be pure MDMA in a suitable dose, MDMA in a too high dose (unlikely, since the illicit dealers like to maximize profit), a mixture with something else, or something else entirely. Who knows? Another problem is the one of bonding with a large number of people, due to the oxytocin release caused by the drug. That can lead to unsafe sex encounters with multiple partners, some of whom might not have the best of intentions.
Then there is the next day. The neurotransmitter 5-HT is supposed to be recycled and taken up again for future use, MDMA sort of cuts off that pathway, flooding the synapses with it and blocking reuptake. Thus, floating free, it is metabolized and eliminated, reducing the natural supply. Most MDMA users exhibit a depressive state for some number of days after the experience, since they are essentially “out” of 5-HT. It finally regenerates, in time for the rave next weekend. But it is not that simple.
Chronic MDMA use, as supported by animal studies, actually damages the neurons that produce 5-HT. Those studies show that the neuron extremities that produce and handle it become swollen and distorted, at least in the short term, and there is no answer to the question if they ever recover. Neurons do have some regenerative abilities, but far from those involved with epithelial cells, for example. There is a better than even chance that long term, high dose use of MDMA will cause permanent brain damage, injuring the very nerve routes that allow for love and good feelings. Some studies have shown that this is, at in part, is irreversible. Not something to fool with, in my opinion.
That means that people who use lots of MDMA, if this research is correct, will never be able to have proper emotions. Yes, it means that. Destruction of 5-HT producing cells in the brain causes that, and depression as well. Oh, pills of shots will not help. 5-HT does not cross the blood-brain barrier, so supplements can not help.
My recommendation is NOT ever to use this drug. I am pretty cool with many, but this one has issues that we have not addressed. The sequalae could be a disaster. Just stay away from it.
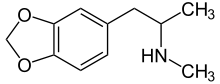
Another interesting one is DMA, sort of the daddy of MDMA. It is just like MDMA, except for the methyl group on the nitrogen. It was popular years ago, and it actually, because of being outlawed in the United States, gave rise to MDMA.
Here is the structural formula. Notice that if differs from MDMA by only that one methyl group on the nitrogen:
MDA
It became illegal earlier than MDMA, and only because it was more popular at the time. It is very similar in effect and toxicity, but for these: it seems to be a bit more hallucinogenic, and less empathogenic. It also is more toxic, with the amphetamine parts of it overcoming the psychedelic parts. I do not recommend it for anyone.
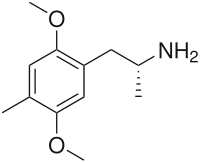
A historical psychedelic amphetamine that is not much found any more is 2,5-dimethoxy-4-methylamphetamine, aka DOM or STP. This material is extremely potent for this class of drugs, 10 milligrams being a very large dose. It is now Schedule I. It also has a very long duration of action, in some cases days, at large doses. Pete Townshend from The Who reportedly took too much in the 1960’s and hallucinated for four days. He swore off all psychedelics after he “came back”. Here is its structural formula:
Now for what is in the market. LSD is purportedly out there, but I suspect that very little of what is sold as LSD actually is. The precursors are closely controlled, and extremely controlled conditions are required to make and preserve it properly. Most of what is marketed as LSD is one of two very potent psychedelic amphetamines, and one or two of them have subjective reactions indistinguishable from LSD except for very experienced users.
Now for what folks in the past couple of decades might likely have ingested, thinking that it was LSD.
There are a couple, and one sounds like the one. It is relatively easy to make, has many of the effects of LSD, and is relatively potent, requiring only 10 to 20 milligrams. It is 2,5-dimethoxy-4-ethylphenethylamine and is called 2C-E. Here is the structural formula:
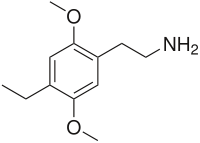
2C-E
Users of 2C-E report odd physical side effects that are not as common with LSD. Muscle cramps and soreness the next day are not uncommon, and users feel the need to move about because of muscle tension, sort of like restless leg syndrome. It also seems to cause more sound distortion than does LSD according to experienced users of both. I would bet that much of the “LSD” on the market today is this material.
Another candidate for “LSD” is 2,5-dimethoxy-4-n-propylthiophenethylamine, called 2C-T-7. Here is the structural formula:
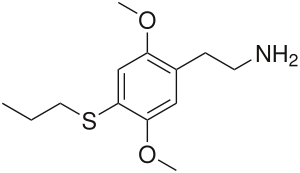
2C-T-7
This material also has some negative physical effects, similar to those for 2C-E. It is also fairly potent, a dose being from 10 to 30 milligrams. This is a Schedule I material and has been associated with some deaths, but other stimulant drugs were also involved in those cases. I suspect that some of the “LSD” on the market today is actually 2C-T-7.
No discussion of this class of drugs would be anywhere near complete without mentioning Dr. Alexander Shulgin. Now 82 (he will be 83 on Tuesday), he personally developed almost all of the psychedelic amphetamines. In addition to developing them, he has personally tested all of his developments as well. So this guy has used psychedelics on a regular basis since the late 1950s and is still kicking. I think that this is fairly good evidence that, used responsibly, psychedelic drugs are not necessarily very harmful. Of course, any damn fool can find a way to hurt herself or himself, but both his and Dr. Hofmann’s history tend to provide support to the idea that these kinds of drugs will not kill you to death immediately.
I could keep going, but I believe that this has covered the subject adequately. For further reading, see if you can find a copy of the book, Phenethylamines i Have Known And Loved: A Chemical Love Story, written by Shulgin and his wife of 28 years, Ann. I recommend that you not purchase this book online, since DEA considers it a “cookbook”.
Well, you have done it again. You have wasted a perfectly good batch of electrons reading the nonsense that I spew. And even though David Letterman expresses remorse when he hears it, I will repeat that I learn much more than I could possibly teach writing this series, so keep those comments, questions (even on other scientific topics), corrections, tips, and recs coming.
UPDATE: Well, I guess Letterman must have read this post since he expressed as much remorse that is possible for him. LOL!
Next time we will discuss the psychedelic indoles (except for LSD, which deserves its own installment). Some of these drugs have been used for centuries, and some are recent.
Warmest regards,
Doc
Crossposted at [dailykos]
24 comments
Skip to comment form
Author
seeing past conventional wisdom?
Remember, recs are also appreciated very much.
Warmest regards,
Doc
Author
recommended this post. I very much appreciate it. More to come, and I already gave some links to past ones.
Warmest regards,
Doc
As a shamanic practitioner who spent several years in childhood prescribed Dexidrine, I find this stuff interesting reading. I was briefly prescribed Ritalin a couple of years back because as my body chemistry is changing during perimenopause the ADD came back with a vengeance, but I stopped using it because after a week or two it became clear that my doctor was more interested in me as a guinea pig and/or cash cow than a patient, and he was trying to ratchet up the pills to a ridiculous degree.
I have never used psychotropics to bring on a trance state, although I have used music, sleep deprivation and the form of sensory deprivation known in my tradition as “going under the cloak”.
I hope you keep going with these essays. Thanks.
Author
for front paging this poor effort. I appreciate it very much.
Warmest regards,
Doc
Translator,
That`s a lot to absorb.
I picked up on a number of references you made to effects & also “day after” effects/results.
The loss of Sodium is something I did not realize was so important & possibly fatal.
As a long time drug user/ abuser, this is a very interesting series, even though this is my first reading of your posts on the subject.
I have to mention that I`m pretty much over my drug use days, except for one of the worst ones, Camel non filters.
One thing I could never understand is how one could eat some pills, sweat a whole bunch, within a writhing mass of people, to the incredibly loud beat of Techno Thrash. And they call them Raves. I`d be a raving lunatic in short order.
(Yes, I have taken Ecstasy & before that DMA, but not on a “can`t wait for Sat. to do it again”, schedule)